|
|
FlakeHQ
Interviews:
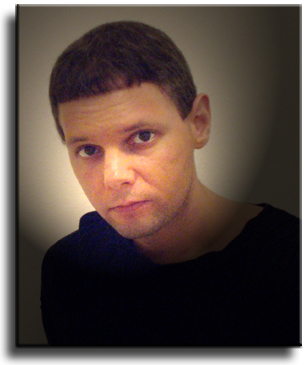
Michael HarnickProprietor/Producer: ShockingPsoriasis.com
Interviewed by Ed
Dewke
***** Dewke: “Shocking Psoriasis” is an aptly-named web phenomenon. What made you decide to produce this web site?
Dewke: My reaction to ShockingPsoriasis.com was immediate and visceral. I kept saying to myself as I clicked through the galleries, “It’s about time!” How does my reaction compare to others from whom you’ve heard? Harnick: I have received a great response to the website so far in this first month it has been up. Many of the reactions people have had are similar to yours: “It’s about time,” or “thank you so much for this website,” very heartfelt and encouraging reactions. Other responses have been exactly what I had anticipated. Some people, including close family and friends, were completely shocked and disturbed by the website, and one close friend could not deal with it at all for about two weeks. What I also found interesting was a “crossover” type reaction I had seen. People with psoriasis, as expected, were generally the ones who were very thankful for the website, whereas the people without the disease were the ones who were most shocked. This was an expected reaction. However, I found it interesting that some of those without psoriasis, had absolutely no problem looking at the pictures or videos, and were not disturbed one bit, whereas there have been some people with psoriasis who were completely shocked by the website. It’s interesting how different we all are, and how we react to different things in life. When deciding to create the site, I really had no idea how people would respond. I did, however, suspect there would be a certain percentage of people whom, after looking at the first few pictures on the home page, would immediately leave because they were just too uncomfortable with the images, and I understand that completely. Skin diseases of any kind, or burns, are very difficult to look at for some people, including myself at times. Over the years, however, I have become so accustomed to looking at my own severe psoriasis, that I am somewhat desensitized to these types of images. I’m always seeking input from other people to try and understand what a “typical” reaction may be from people viewing the website for the first time, or viewing new pages or videos that I may be working on. I think the most effective galleries so far, are not the ones showing the psoriasis on the different areas of the body, but the pictures of the bed sheets in the morning with all the dead skin, and the sink and bathtub images with the psoriasis scale and blood. I suspect those images have a strong impact on people, particularly those just starting to learn about psoriasis and other aspects of the disease.
Dewke: Why do you suppose it’s taken so long for a show-&-tell site like yours to materialize on the web? Harnick: Three words: embarrassment, isolation, and depression. Depending on the severity of the condition, psoriasis can be an extremely isolating disease, which can frequently lead to depression, particularly when it becomes severe in visible areas. I think people are ashamed and embarrassed because of their psoriasis, at least I was, and the last thing they would ever think of doing would be to put themselves on “display” on the Internet. I understand this completely. I felt that way for so many years living with this disease, I would never show my skin to anyone, even close family. As I mentioned earlier, this attitude of mine has changed only over the last year or so. I am now more comfortable showing my skin, as demonstrated by the website — but in my everyday life, I still tend to cover up. The difference now is that I’m no longer ashamed of who I am because I have this disease, and my attitude now is basically, if someone can’t handle my psoriasis, or they have a problem associating with me because of the psoriasis, then it’s their problem, not mine. I am more than happy to do whatever I can to educate people about psoriasis, show them the lesions, talk about treatments, etc., but in the end if they’re just too uncomfortable with it, or with me, then it’s just not my problem, and most importantly, I no longer feel bad or ashamed about the fact that I have psoriasis.
Dewke: Should people with mild psoriasis look at ShockingPsoriasis.com? Why (or why NOT)? Harnick: This is actually one of the main questions I had in mind before deciding to go ahead and develop the site. The majority of people have mild to moderate psoriasis, and I was trying to gauge the response that they might have to seeing very vivid images and videos of severe psoriasis. The website, as you know, is very graphic, and may be quite disturbing for many people, both with and without psoriasis. The only way I could approximate what a typical reaction might be, was to try and think back when I had only the mild form of the disease, and how I might react if I came across a website like this. Being completely honest with myself, I don’t think I would have wanted to see a site like this when my psoriasis was just beginning, out of the fear that I may someday look like that guy. I don’t think that was something that I would have been able to deal with it at that point. Some people have mild psoriasis all of their lives. It never progresses into anything further. They have learned to deal with a few patches here and there that are controlled most likely by topicals, and they go on with their lives. These are the people who I think would be the least interested in the site, because they are well adjusted to their psoriasis and, let’s face it, nobody enjoys looking at a severe skin disease. For people with active psoriasis that is worsening, they may have much more of an interest in viewing the site, and seeing what they themselves may be dealing with in the future. Again, looking back at the point that my psoriasis was progressing from the mild to moderate, and then from moderate to severe, I would have loved to see a website or video or book that vividly demonstrated and explained exactly what was involved, just to prepare myself mentally for the challenges that I may face with this disease. These are the people I had in mind when deciding to create the site. And for people with severe psoriasis who view the site, I think it becomes somewhat of a “thank God I’m not the only one going through this” type of response. Not that they’re glad to see other people with the disease, but because they at least now know that there are other people out there going through the exact same issues and challenges. For people without psoriasis, my intention was to help bring increased awareness and understanding to this disease in hopes of mitigating some of the typical negative reactions people have when confronted with a person with psoriasis. I have no idea if I will be successful in this attempt, there’s no way for me to know exactly how many people viewing the site, have or don’t have psoriasis, but it was another main reason for producing the website.
Dewke: Tell us a little more about your own case. How old were you when your psoriasis erupted? How did it start and what did you experience on the road to the "you" we see in the photos and videos? The treatments you've tried (http://www.shockingpsoriasis.com/mypasttreatments.html) are pretty comprehensive. (I think what you have NOT tried would have been a shorter list!) Harnick: I can remember as far back as age fourteen when I first experienced mild symptoms of what I now know was psoriasis. I had a little redness and flaking behind the ears, and some flaking on my face. At that time however, being a teen, I was battling pimples, and I had probably just assumed that any flaking or redness was the result of having acne, not psoriasis. I was officially diagnosed with psoriasis around eighteen or nineteen when I was in to see my dermatologist for a normal check up for the acne, and he had noticed a few small psoriasis lesions on my eyebrows, and asked if I had any problems elsewhere. I showed him some small patches behind the ears, and the scalp line, and he told me that I have psoriasis, and gave me my first prescription for topical steroids, I believe it was Elocon. The dermatologist told me to use the topical steroid sparingly because of skin atrophy and other side effects. For the next four to five years, through college, the psoriasis slowly progressed from mild to moderate, or about 6-10% coverage, spreading from my scalp and eyebrows, to other areas of my face, legs, genitals, and butt. The treatment at this point was simply more topical steroids, and a new topical called Dovonex, which was not a steroid. Now instead of one topical medication, I had a few of them for different areas of the body. I recall I was given Diprolene for the legs and butt, Desowen for the facial and genital areas, and continued with the Elocon for the scalp and eyebrows, and Dovonex to be applied everywhere but the scalp.
I remember one visit to the dermatologist, when I was in the early stages of severe psoriasis, who sent me home with six prescriptions for topical medications: four steroids, a prescription tar lotion, and another new topical called Tazorac, which took the place of the Dovonex that hadn't worked. I remember filling all of them at the pharmacy, and the cost came to something like three or four hundred dollars, it was ridiculous, and I would have to refill them once a month because the psoriasis was becoming more and more widespread. It was at this time that I chose to educate myself about psoriasis and all of its treatments, so I bought a PDR (Physicians Desk Reference), and turned to the pages that listed all the treatments for psoriasis. I learned some of the medical jargon, enough to understand what I was reading, and learned there were very limited medications available for the treatment of psoriasis. Besides topical medications, there were really only two medications available, both of which are potent, and had a very scary side effect profile. These are methotrexate and cyclosporine, which were originally prescribed for chemotherapy and organ transplants, respectively. Also, by this time, I started to see many of the side effects of the topical steroids: skin atrophy, striate marks (purple stretch marks), as well as a very fast and aggressive rebound effect which caused the psoriasis to become completely out of control, covering nearly 60% of my body. I was basically using steroids all over my body and face, and using them with an occlusive dressing, particularly the very potent ones such as clobetasol, that should NEVER be used with an occlusive wrap. Things were also starting to breakdown in my relationships as well, as I was choosing to become more and more isolated because of the embarrassment of my condition, particularly on my face. I was becoming more and more depressed. So I went back to my dermatologist and asked him about methotrexate and cyclosporine, and he said it was a “sledgehammer” approach to treating psoriasis because of the potency and immunosuppressive activity of these drugs. He did tell me a little bit about light treatments, and PUVA, but he didn’t offer them, instead he suggested a guy in the New York City who offered light treatments. I wasn’t going to travel sixty miles into NYC three times a week for a 30 second zap in the light therapy box. So I began to sink deeper and deeper into depression which I’m sure had a detrimental effect on the psoriasis. Over the next year or so, my psoriasis was flaring so bad, to a point of 90-95% coverage, including my face. I had lost all of my friends, my girlfriend had found someone else because she couldn’t deal with me anymore. I was out of money and couldn’t hold a job because I was literally shedding skin and blood everywhere. I was in tons of debt, and it was at this time that I basically gave up, and began to plan a suicide. This continued for another four months or so, and my family in NY noticed that something was very wrong. I was extremely and dangerously depressed. It was at this time that my mother called my father in Florida, and I was on a plane to Florida within days to try to get the needed treatment. Once in Florida, we eventually found a great dermatologist who specialized in psoriasis, and it was then that I began light treatments, specifically PUVA along with Soriatane. After about 12 weeks of treatments, all I had left of the psoriasis was some minor redness where the plaques used to be, and by the fifth month I was completely clear of all psoriasis. I had my life back. Found a job, an apartment, put some money in the bank, had some stability. And then I was diagnosed with Psoriatic Arthritis, and the real battle began. As bad as your skin can get from psoriasis, your joints can become just as bad. The arthritis first began in my toes with a couple of “sausage digits,” as they are called. Over the next four years, just like the skin psoriasis, the arthritis went very aggressively from mild to severe, to the point of total disability. It was this period up until present day, in which I’ve tried all of the systemic medications that are listed on the My Past Treatments section of the website. This is an incomplete list as there are many other medications that I’ve used, such as different NSAID’s, other off-label immunosuppressant drugs, muscle relaxants, strong narcotics such as oxycodone, morphine, and Duragesic (fentanyl) patches, the so called “dirty” tricyclic anti-depressants, and even antibiotics. Psoriatic arthritis has proved to be a much greater challenge for me at this point. Now I’m dealing with the challenge presented by just walking on top of a severe psoriasis flare on my skin. I am currently awaiting a phase II drug trial through Bristol-Myers Squibb for Orencia, which is currently approved for the treatment of Rheumatoid arthritis, and is being studied for the treatment of psoriatic arthritis. Maintenance medications that I am currently on include limited topical steroids, Diclofenac, and Oxycodone, but I am considering starting light treatments again despite skin damage, if for some reason the Orencia doesn’t come through.
Dewke: What do you believe triggers your P? Also, what do you think about alternative therapies including diet, dietary supplements, climatotherapy ... ?
I’ve heard of some people, whose psoriasis regularly comes and goes depending on different factors such as stress, diet, depression, etc., but that once these factors are addressed or eliminated, their psoriasis tends to subside. This has never been the case for me. I’m both flaring and getting worse every day or it’s under control from a specific treatment. The psoriatic arthritis however, is much more unpredictable, and really all over the map. When I’m in a severe arthritic flare, the arthritis is constantly rotating from body part to body part, which can last anywhere from days, weeks, or months, it’s really bizarre. For example, I could be going along with a major flare in my back and right foot, for three months, and then out of nowhere, the pain and inflammation completely disappears, but now I have severe pain or swelling in my right hand and two fingers, and my left SI joint, which may only last a week, and then it‘s on to something else. It’s like the inflammatory molecules, or TNF-alpha proteins, or whatever they’re called, are just roaming around my bloodstream, and they get bored of inflaming certain areas, so they decide to close up shop and move to a new residence. Sometimes however, I will have a flare in a particular body part that lasts for months and months without any relief whatsoever. This is my current situation, where my left foot has been swollen and inflamed, and has actually become deformed to some extent, and this has been going on for nearly eight months now. Regarding alternative therapies, I have tried nearly every diet proposed to alleviate psoriasis and arthritis symptoms, and have taken many different supplements, and I’ve never found any relief from any of them. I’ve tried fish oil, evening primrose oil, selenium, zinc, tumeric, all banana diet, all veggie diet, all protein diet, no protein diet, all carb and no carb diets, and finally no diet. No diet, or fasting for about one week, is the ONLY “natural treatment” that has ever helped my psoriasis. Obviously this treatment method has some flaws — starvation, for instance — but it did help a bit. I’m not sure if this one qualifies as climatotherapy, but the craziest thing I’ve ever tried was taking a magnifying glass in the sun, and concentrating the light on a psoriasis lesion to try and “simulate” light therapy treatments. (I didn’t have medical insurance or enough money to pay for the real thing.) Sometimes we psoriatics get desperate, and I could probably rattle off a few more crazy things I’ve tried, but it’s just not necessary. I have heard that some people get relief from the Pagano diet, which I have tried a few times, but never had the discipline to stick with. Personally, I have no problem with trying new medications or treatments. I no longer worry about the side effects from potent systemic medications, and I have no problem offering myself up as a guinea pig in pursuit of new treatments. This, I’m sure, is an unpopular viewpoint, as there once was a time that I myself also feared trying various medications because of all the potential short term and long term side effects. Eventually, however, I got to a point where I needed to focus on my current quality of life, and not live in fear of all the potential side effects or other problems that I may encounter down the road. I can only live day by day.
Dewke: Some of us are surprised by your willingness to participate in drug trials. What if you get put in a control group and effectively get NO treatment for some time? Or what if the drug doesn't work for you? It sounds like your flares — both skin and joints — can be debilitating, or at least much worse than an inconvenience. Are you able to establish some limits on how bad things can get before you drop out and return to a therapy you know can help? Harnick: There are a few reasons why I’m willing to participate in drug trials without any apprehension. First, with regards to the psoriatic arthritis, there are literally no other treatments available for me at this time, I have been on nearly all of them, including many off-label drugs not listed in the "My Pasts Treatments" section of the website. I’ve also been on many combinations such as MTX (methotrexate) and Enbrel, MTX/Remicade, MTX/Humira, MTX/Cyclosporine, MTX/Imuran, among others. They like to combine methotrexate with everything. A few worked for a little while, one worked for over a year, and the rest either did not work, or I could not tolerate the side effects. So I basically have no other options at this point. As mentioned in a previous question/answer, the arthritis is much more troubling for me right now, as it’s very difficult for me to walk and get around. I actually went shopping for a cane a few weeks ago, but just couldn’t buy it. I’m stubborn, and I just don’t feel comfortable being in my early thirties, and having to walk around with a cane. Am I being vain about this? Yes, I probably am, but this is another obstacle in my life that I’m going to have to come to terms with. So as bad as my psoriasis currently is, being able to walk is more important for me right now. Now, as far as the risks of participating in drug studies, I’m not concerned with this matter one bit. The reason is, almost all of the drugs approved or being studied for Psoriatic arthritis, have already been approved for Rheumatoid arthritis, and are currently available. The reason for this is simply money. More people have rheumatoid arthritis than psoriatic arthritis, so the drug companies will look to study the medications in the group with the largest potential “customer” base before conducting studies in less common diseases. This should come as no surprise, it’s simply maximizing profits. The advantage of this, at least for the people with psoriatic arthritis or other less common diseases, is simply that, because the medication has already been tested, approved, and is currently on the market for rheumatoid arthritis, the likelihood of encountering severe side effects when studying it for psoriatic arthritis is very minimal. Drug companies are required to conduct separate studies for each condition they’re looking to treat, even though it has already been approved for a similar disease(s). Of course the physician could just prescribe it off label, but because the drug is not yet approved for psoriatic arthritis, insurance companies won’t pay for it, and, as you know, the cost of the biologics and other new medications are astronomical, so paying out of pocket (at least for me) is not an option.
Finally, most of the systemic medications studied and approved for psoriatic arthritis, also work to some extent for the psoriasis. However, not all of the drugs approved or studied for psoriasis, work for psoriatic arthritis, such as Amevive, Raptiva, and Soriatane. I’d rather try to kill two birds with one stone by focusing on the medications for psoriatic arthritis.
Dewke: You’ve been very candid about your bout with depression. Did you ever seek specific help for that? Many psoriatics go through it. What advice do you have for them? Harnick: I didn’t really willingly seek help, but yes I did end up seeing someone, and was put on some anti-depressants to treat the depression. After moving down to Florida, I was put on Paxil for six months, and then three years later, when the psoriasis returned once again (~80% coverage), I was given Zoloft, and then Wellbutrin.
Dewke: Have you got any long-range plans for ShockingPsoriasis.com (that you're willing to share ahead of time)? What are you working on now? What will we find there next? Harnick: I have a number of new ideas that I’m currently working on, or at least starting to think about. I will definitely be adding more videos to the site, some graphic, but many in which I will just be talking about some aspect of psoriasis or arthritis, based on my experiences of living with the disease. I have received a number of requests about creating a “Guest Flakers” section, where people would be able to submit their own pictures and perhaps a brief bio about their own experiences with psoriasis. I would like to create a “Psoriasis/Psoriatic Arthritis Research” section that would be continuously updated, and would include a listing of all the current and future medications and treatments being studied, along with articles, news items, results from drug trials, and other information relating to psoriasis. I have also received a number of emails and requests from people who would love to see a “Results” or “Before and After” section or gallery in which I would showcase my improving (hopefully) skin, once I get back on a treatment such as the Orencia or other medications or treatments. People are reporting they would love to see the transformation from 70 to 80% coverage to completely clear skin documented with images and/or video, and, needless to say, I'd love to provide that transformation and coverage! I have plenty of other ideas, but you’re going to have to keep visiting the website to find out!
Dewke: And indeed I will, Michael! Thank you for taking the great amount of time your responses have no doubt required, but more importantly, thanks for ShockingPsoriasis.com. You have fulfilled (and are fulfilling) a need. ***** * Poems, Alan Dugan, "The Yale Series of Younger Poets", ©1961 Alan Dugan, p.12 (Oxford University Press)
##### www.flakehq.com |

 So
I had reached the point where I had enough of being embarrassed or
feeling ashamed because I had this disease, and I literally went from
one extreme to the other. Not only did I no longer have a problem
showing the psoriasis lesions on my body, but I wanted to take it a step
further and show everybody the actual removal of the psoriasis scale and
blood, and document what daily life is like for someone who is basically
“shedding” skin all day. I wanted to show what it was like waking up
every morning to a pile of dead skin, stuck to the sheets because of the
dried seeping blood. Or the chunks of dead skin and blood left on the
bathtub floor after taking my morning shower. I knew that many of these
images may be quite disturbing or shocking for many people, especially
those without the disease, and it was from here that I came up with the
domain name ShockingPsoriasis.com, which I thought was accurate
and pretty easy for people to remember.
So
I had reached the point where I had enough of being embarrassed or
feeling ashamed because I had this disease, and I literally went from
one extreme to the other. Not only did I no longer have a problem
showing the psoriasis lesions on my body, but I wanted to take it a step
further and show everybody the actual removal of the psoriasis scale and
blood, and document what daily life is like for someone who is basically
“shedding” skin all day. I wanted to show what it was like waking up
every morning to a pile of dead skin, stuck to the sheets because of the
dried seeping blood. Or the chunks of dead skin and blood left on the
bathtub floor after taking my morning shower. I knew that many of these
images may be quite disturbing or shocking for many people, especially
those without the disease, and it was from here that I came up with the
domain name ShockingPsoriasis.com, which I thought was accurate
and pretty easy for people to remember. Looking
back, I deeply regret being given so many steroids, because it would
later prove to be one of the contributing factors to my psoriasis
developing into the severe form of the disease. By twenty three, I had
found someone that I was planning on marrying at some point, who also
had some mild skin problems, (not psoriasis) and could relate to my
increasing tendency of wanting to cover up all the time, even in the
summer time. I had graduated college with a degree in music theory and
performance, and was teaching piano and guitar privately and through a
local music store (no medical benefits, but plenty of credit cards to
continue to buy those $100+ tubes of topical medications).
Looking
back, I deeply regret being given so many steroids, because it would
later prove to be one of the contributing factors to my psoriasis
developing into the severe form of the disease. By twenty three, I had
found someone that I was planning on marrying at some point, who also
had some mild skin problems, (not psoriasis) and could relate to my
increasing tendency of wanting to cover up all the time, even in the
summer time. I had graduated college with a degree in music theory and
performance, and was teaching piano and guitar privately and through a
local music store (no medical benefits, but plenty of credit cards to
continue to buy those $100+ tubes of topical medications).  Harnick:
I really can’t accurately say what triggers a flare, but I
definitely know what aggravates it, and significantly worsens it. The
Keobner Phenomenon brought on by the overuse of topical steroids, plus
stress, depression and alcohol have always been the main culprits. For
me, once the psoriasis becomes active again and begins to flare, if left
untreated, it will continue to worsen to the point that I am about
eighty or ninety percent covered.
Harnick:
I really can’t accurately say what triggers a flare, but I
definitely know what aggravates it, and significantly worsens it. The
Keobner Phenomenon brought on by the overuse of topical steroids, plus
stress, depression and alcohol have always been the main culprits. For
me, once the psoriasis becomes active again and begins to flare, if left
untreated, it will continue to worsen to the point that I am about
eighty or ninety percent covered.  Concerning
the potential of being put in the control group, there is always that
possibility. Doctors speak of the placebo effect frequently, and my
rheumatologist told me that around 30% percent of trial subjects respond
positively to the placebo (that is, they exhibit the placebo effect).
However, for the placebo effect to work, you have to first believe that
you are actually getting the medication, not the placebo, and also
believe that the drug is going to work and help you get better. I,
however, being cynical when it comes to these things, will take the
opposite approach. I will assume that I am getting the placebo instead
of the drug, and therefore also assume that there is absolutely no
chance of getting better. Now this sets up two possible scenarios. If I
don’t see any response within a reasonable amount of time (1-2 mos.),
then either the drug did not work, or I was right and I did in fact
receive the placebo, in which case I will drop out of the study. If
however, I do see a response, then I know I got the drug, and will
happily remain in the study. Because I have essentially “inactivated”
the placebo effect by assuming I got the placebo in the first place,
then I know where I stand with regards to whether I want to continue
with the study or not. Sounds a bit convoluted, but it’s accurate. So to
answer your question directly, my cut off date is about six to eight
weeks. Two months is by far enough time to see at least a minimal
response.
Concerning
the potential of being put in the control group, there is always that
possibility. Doctors speak of the placebo effect frequently, and my
rheumatologist told me that around 30% percent of trial subjects respond
positively to the placebo (that is, they exhibit the placebo effect).
However, for the placebo effect to work, you have to first believe that
you are actually getting the medication, not the placebo, and also
believe that the drug is going to work and help you get better. I,
however, being cynical when it comes to these things, will take the
opposite approach. I will assume that I am getting the placebo instead
of the drug, and therefore also assume that there is absolutely no
chance of getting better. Now this sets up two possible scenarios. If I
don’t see any response within a reasonable amount of time (1-2 mos.),
then either the drug did not work, or I was right and I did in fact
receive the placebo, in which case I will drop out of the study. If
however, I do see a response, then I know I got the drug, and will
happily remain in the study. Because I have essentially “inactivated”
the placebo effect by assuming I got the placebo in the first place,
then I know where I stand with regards to whether I want to continue
with the study or not. Sounds a bit convoluted, but it’s accurate. So to
answer your question directly, my cut off date is about six to eight
weeks. Two months is by far enough time to see at least a minimal
response. I
have to be honest here, the antidepressants did not help me one bit, and
logically there’s no reason why they should.. My problem is simply the
fact that I’m shedding skin and blood everywhere I go, and have chronic
pain many days of the year, and my depression (or lack thereof) is
directly related to the severity of my symptoms. Obviously I feel the
best when I’m clear, and the worst when I’m covered with psoriasis
and/or in pain, and antidepressant medications do not change this fact.
Again this has just been my experience. I’m not against antidepressants
in anyway, they have just never worked for me. If someone thinks that
they might help with their own depression I think it‘s a good idea to
try them. I have a family member who has had MS (Multiple Sclerosis) for
many years, and she takes Zoloft when she’s going through a bad episode,
and I believe it has always worked well for her. So everybody’s
different. For me, until I‘m covered around 50% or better, the psoriasis
no longer depresses me that much, I’m so used to it. But it's taken many
years for me to get to this point. The arthritis tends to get me down
more, mainly because it is much more disabling, and being on
round-the-clock pain medications can’t help, as it just drags your
overall mind and body down. I have learned over the years to just
concentrate on what I have to get done for today, and not to constantly
worry about all the what-ifs I may have to deal with down the road. I’m
usually happier when I approach life like this, but like everyone else,
I have my moments, and when the psoriasis grows beyond 50 or 60%
coverage, all bets are off.
I
have to be honest here, the antidepressants did not help me one bit, and
logically there’s no reason why they should.. My problem is simply the
fact that I’m shedding skin and blood everywhere I go, and have chronic
pain many days of the year, and my depression (or lack thereof) is
directly related to the severity of my symptoms. Obviously I feel the
best when I’m clear, and the worst when I’m covered with psoriasis
and/or in pain, and antidepressant medications do not change this fact.
Again this has just been my experience. I’m not against antidepressants
in anyway, they have just never worked for me. If someone thinks that
they might help with their own depression I think it‘s a good idea to
try them. I have a family member who has had MS (Multiple Sclerosis) for
many years, and she takes Zoloft when she’s going through a bad episode,
and I believe it has always worked well for her. So everybody’s
different. For me, until I‘m covered around 50% or better, the psoriasis
no longer depresses me that much, I’m so used to it. But it's taken many
years for me to get to this point. The arthritis tends to get me down
more, mainly because it is much more disabling, and being on
round-the-clock pain medications can’t help, as it just drags your
overall mind and body down. I have learned over the years to just
concentrate on what I have to get done for today, and not to constantly
worry about all the what-ifs I may have to deal with down the road. I’m
usually happier when I approach life like this, but like everyone else,
I have my moments, and when the psoriasis grows beyond 50 or 60%
coverage, all bets are off.